Forty years ago, a machine meant to help save lives administered a massive overdose of radiation to patients undergoing vital treatment. In some cases, this proved fatal – and avoidable software programming errors were to blame.
Words by Lachlan Haycock
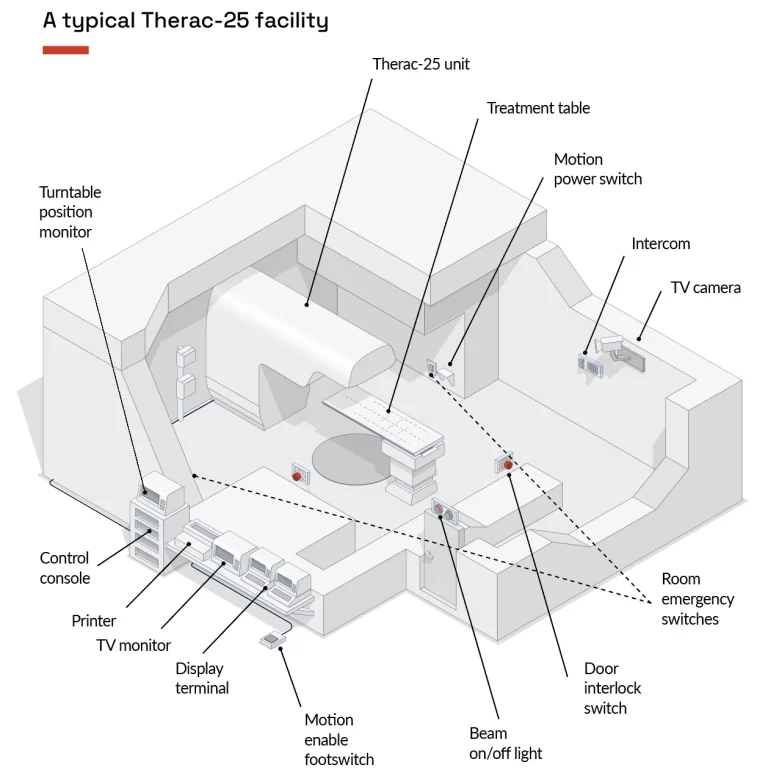
On 3 June 1985, a 61-year-old woman in Georgia, United States, was receiving follow-up radiation treatment after a lumpectomy to remove a malignant breast tumor. The radiation machine involved in the procedure was a Therac-25 unit produced by Atomic Energy of Canada Limited (AECL), and one of 11 units that had been installed across Canada and the US.
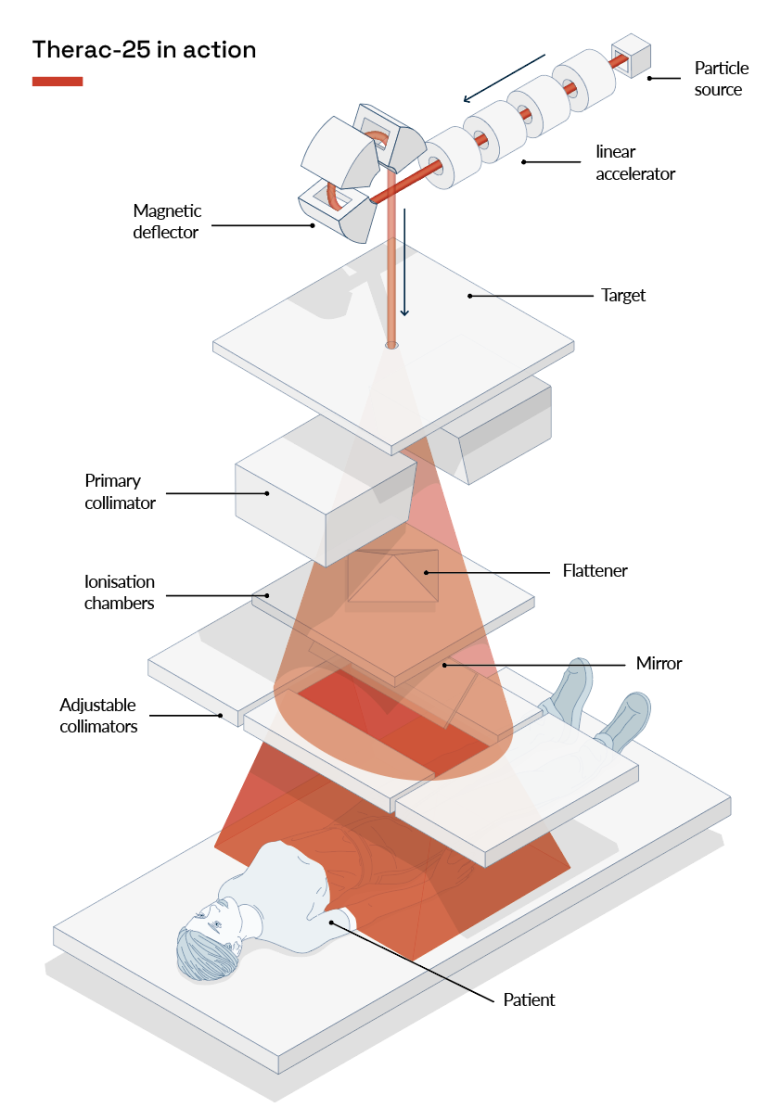
The patient was set to receive a 10 megaelectron volt dose (or 10 million electron volts) to the clavicle. She later reported that, after the machine was turned on, she felt a “tremendous force of heat” and a “red-hot sensation” near the treatment area. Afterwards, although the skin was warm to the touch, no marks were visible.
On 26 July 1985, a 40-year-old woman receiving treatment for cervical cancer in Ontario, Canada, reported feeling a burning sensation, or “tingling shock”, in her hip following a dose from another Therac-25. The machine had initially shut down and displayed an error message, leading the operator to make five successive attempts at restarting it to administer the dose.
Following the fifth attempt, the machine shut down and a hospital technician was called, but did not identify any fault in its setup. Four days later, the patient was hospitalised with burning and swelling in the treatment area.
Crucially, the lack of hardware interlocks or supervisory circuits meant bugs in the software were not identified, leading both patients to receive fatal radiation overdoses. In the case of the Georgia patient, this totalled 20,000 rad. Therac-25 machines were linked to at least four other similar incidents until 1987, when the units were recalled for inspection and modification. Of the patients who received an overdose, four died and two were left with lifelong injuries.