Medical equipment company ResMed, for instance, began when Professor Colin Sullivan at the University of Sydney partnered with Dr Peter Farrell from the Baxter Centre for Medical Research (BCMR).
Farrell, who held a PhD in chemical engineering and bioengineering from the University of Washington, Seattle, and a Doctor of Science from the University of New South Wales, developed a prototype of Sullivan’s nasal continuous positive airway pressure (CPAP) technology.
He conducted clinical trials and then founded ResMed after buying the rights from BCMR, bringing CPAP to the market.
Then there were the late David Robinson’s contributions to the area of diagnostic ultrasound.
This electrical engineer removed untold levels of danger from the childbirth process when he and George Kossof, in the Ultrasonic Research Group of the Commonwealth Acoustic Laboratories, recorded the country’s first ultrasound image of a fetus by using a scanner they had built in their labs.
Such machines had been developed and used elsewhere, but the images from Robinson’s device were far superior and were soon recognised as the future of pre-natal imaging.

Australian researchers have even played an important role in the development and improvement of pacemaker technology.
In 1969, Australian electrical engineering firm Telectronics was the first to use integrated circuits in early pacemaker technology. It also devised the first hermetic titanium encapsulation for pacemakers.
This solved a serious reliability problem caused by the diffusion of water vapour from body fluids through the previously epoxy resin case of the pacemaker.
Decades earlier, in 1926, Dr Mark Lidwill at Royal Prince Alfred Hospital and University of Sydney physicist Edgar Booth built a rudimentary device that could be plugged directly into a power point, with one electrode attached to the skin and another to a needle, which was plunged in to the cardiac chamber.
It was, many argue, the world’s first portable artificial pacemaker.
Dr Graeme Sloman from Royal Melbourne Hospital has also been widely honoured for the work he conducted around developing an implantable pacemaker. The past achievements of Australian researchers and engineers in the biomedical field are enormous. The good news is that it’s not just about the past.
Exciting developments are happening right now and will continue into the future.
Print me a ribcage!
After suffering mild injuries from a jet ski accident at the age of 17, American student Penelope Heller had scans that revealed a growth on her sternum.
It was a rare bone cancer that required the removal of her sternum and of part of her rib cage.
The materials in the implanted prosthetic — Gore-Tex and bone cement — caused her considerable pain in the years after the procedure, so she and her family began looking for a better option.
They came across a story of a 54-year-old Spanish man who, a few years earlier, had faced a similar issue and had devised a solution in consultation with Anatomics, an Australian biomedical business.
It involved 3D-printing a sternum and rib cage using titanium and a porous polyethylene material.
It worked for the Spaniard, and after a negotiation with the US Food and Drug Administration to have the process approved in the United States, it also worked for Heller.
The chief editor of one medical journal referred to the 3D-printing process as the “skeletal wonder from Down Under”.
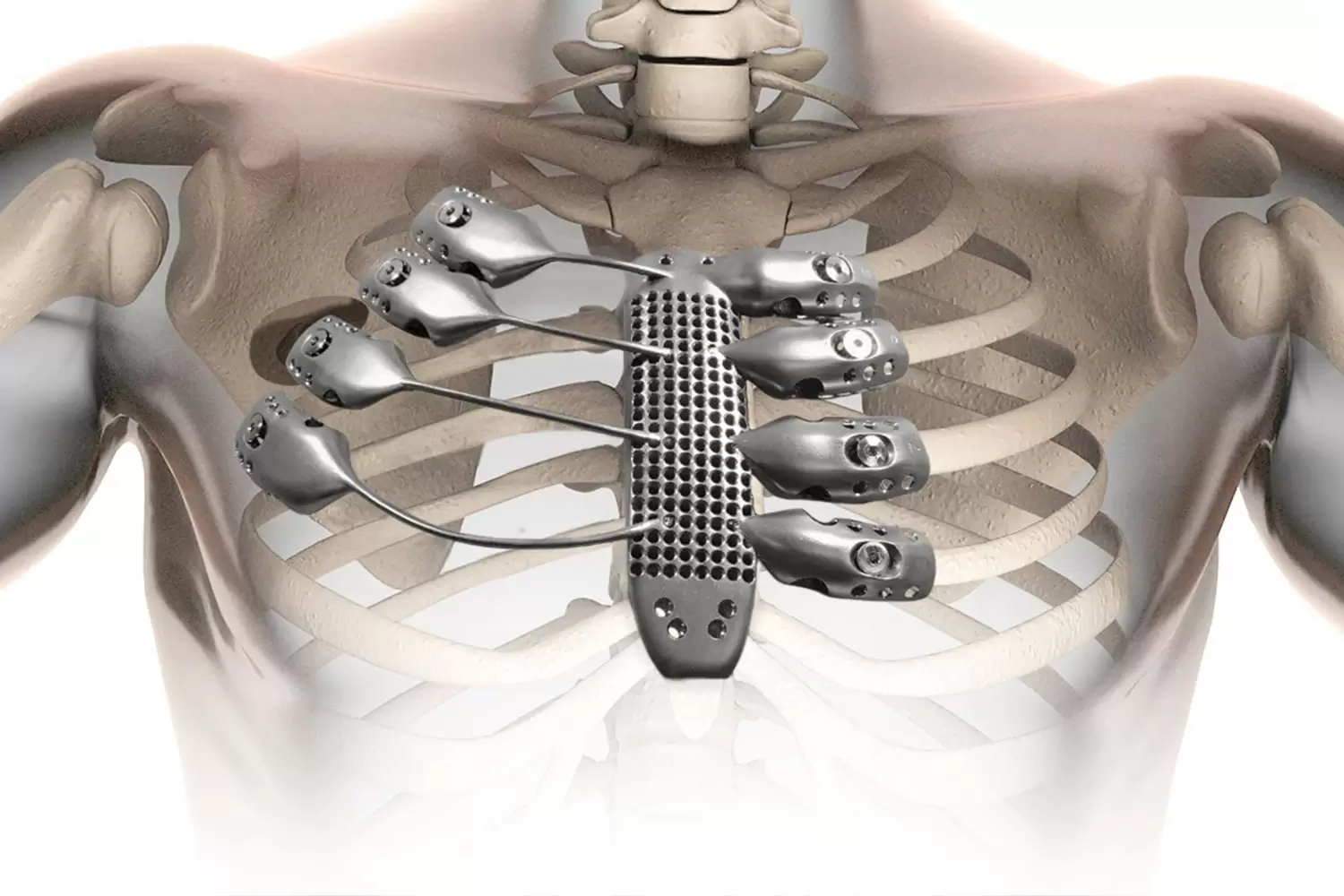
Anatomics works with CSIRO’s Lab 22, a centre for innovation in metallic additive manufacturing. Lab 22 produced the 3D-printed prostheses for both patients.
“We are absolutely punching above our weight internationally,” said Stefan Gulizia, Research Group Leader in the Manufacturing Business Unit at CSIRO. Gulizia, a mechanical engineer, is responsible for Lab 22.
“Five years ago, there wasn’t a titanium additive manufacturing industry in Australia. We have now almost completed the entire value chain, from powder to product,” he said.
“We’ve developed technologies that manufacture titanium powder, technologies that shape that powder and technologies that consolidate the powder into sheet, pipe, wire and complex shapes. We’re developing an entire range of technologies and are also managing the licensing options for Australian companies.
“Sometimes we have equity in these companies, so benefits are coming back to Australia and to CSIRO. We’re really making a difference to the international biomedical industry and to the Australian manufacturing industry.”
As an example, Gulizia mentions Oventus, a business that developed new technology for a sleep apnoea device, but with a design that had to be 3D printed because it is customised for each individual. Oventus and Gulizia’s team within CSIRO partnered to make the design a reality.
CSIRO scientists are inventors of one of the patents, and, in partnership with CSIRO’s Data61 and Lab 22, Oventus is developing the next generation of sleep apnoea devices.
“Data61 helped Oventus develop software that a clinician can use to upload a master file of that sleep apnoea device and manipulate it to fit a CT scan of the specific patient. It’s then sent to be 3D printed.”
A high engagement industry
Is it challenging to 3D-print items that have to go into a person’s body, such as the rib and sternum structure?
In terms of accreditation, Gulizia said, it’s far less challenging to develop a solution for the human body than it is to create a part for the aerospace industry.
“If you’re 3D-printing a part for aerospace it could be a 10-year accreditation process,” he said.

“The medical part may take half that time. CSIRO has equity in the only advanced commercial ARCAM Q10plus EBM 3D printer in Australia with ISO 13485 accreditation, so that makes it a little easier for us.”
In terms of job satisfaction, Gulizia said nothing beats being a part of an engineering process that improves people’s quality of life.
“I haven’t met a scientist in the biomedical field who doesn’t have a high level of excitement about helping people,” he said.
“CSIRO participated in saving a man’s leg recently by developing a customised, titanium heel, printed in our ARCAM machine. It’s very satisfying on a personal level and also in terms of creating new technologies and industries.
“Our research projects in developing new products and processes that go towards supporting productivity gains, boosting sustainability and helping capture emerging opportunities in local and global markets are employing the next generation of scientists and engineers.”
Q&A with Dr Ali Almasi
Dr Ali Almasi, neural engineer at the National Vision Research Institute, speaks with create about how bionic vision is being developed.
create: How close are we to perfecting a bionic eye implant?
ALI ALMASI: We have a prototype that is working, and it has even given some sense of vision to patients. But in terms of vision it is very crude and low resolution. We need to build an electrode array allowing very high-resolution stimulation of retina. We will get there in the near future.
create: Is the challenge technological or medical?
AA: I am an engineer so I can’t give that perspective accurately. In terms of implanting the device into the eye, I don’t think there is a problem with that. There are two ways of approaching the implant.
One is to implant the device into the eye and stimulate the retina to transmit visual information to the brain using the optic nerve. The other is to implant a device into the brain to stimulate its visual area directly.
The team in Australia is pursuing the first approach, which can have less complications since it does not involve open brain surgery.
create: Is Australia leading the way?
AA: Absolutely! Australia has been a pioneer in bionic devices, particularly the cochlear implant.
This article originally appeared as “Life force” in the June 2019 issue of create magazine.