

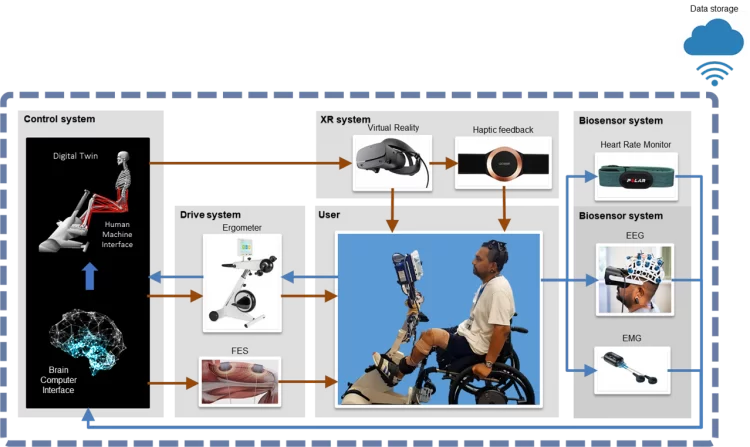
That signal is then transmitted to the ergometer to enable the desired movement — in this case, cycling — to be performed. The system also stimulates the muscles themselves, as would happen organically in the case of someone with an undamaged spinal cord.
“That is basically three components: the brain, the computer model to transform the thought into controlled signals for the devices, and then the devices themselves,” Pizzolato said.
But to make this work requires the technology to mimic a lot of bodily functions we do not usually notice. A cyclist does not think about every contraction of their muscles required to move; they think of the cycling action and allow the specific signals required to make it happen to fire from the spinal cord, and then adjust their movement according to the sensations they feel in their legs.
“Part of the technology involves stimulating the muscles so that there’s a thought-provoking process, of course, as well as actual [functional electrical stimulation] of the muscles,” said Dr Laura Diamond, a biomedical engineer on the team. “We want to understand that feedback loop: how much stimulation is required, how much is safe.”
A customised twin
This is a complex system, and to make it all work, a digital twin is integrated into the technology.
“It’s a computational model of the nervous system, the muscular system and the skeletal system of the person,” explained Pizzolato. “That allows us to translate these signals into something appropriate for the rehabilitation devices that is consistent with how the person would actually move.”
“It’s actually a clinical problem as much as it is an engineering problem,” Diamond said. “People with spinal cord injury, because they don’t have that sensory feedback loop, that can often result in injuries, over-training.”
That’s because they cannot rely on feedback from their nervous system to tell them if something has gone wrong.
“Without that feedback, we need to rely heavily on the computation, and the digital twin is what we’re actually able to do that with,” Diamond said.
The ultimate goal of this is rehabilitation: the hope is that the patient will be able to regain at least some control over the paralysed portion of their body.
“By combining the downward signals from the brain down and upward from muscles and tendons back up, there is evidence that it promotes neuroplasticity,” Pizzolato said.
“That enables reconnection of neurons within the spinal cord, as well as neuroplasticity, meaning that these signals can be redirected through still intact pathways back to the brain.”
That’s based on pre-existing research showing that such connections are possible to form, and the digital twin is designed to adapt once the patient has regained some control.
“At the moment, Dinesh doesn’t have any voluntary control of muscles in his lower limb; he’s relying fully on stimulation,” Diamond said. “But the assumption is that when that changes, we would then want the stimulation to adapt depending on how much he was actually contributing to the cycling.”
Expert insight
BioSpine is now undergoing its first round of clinical trials and, as well as leading the team, Palipana is currently its sole test subject. Using his experiences and expertise, they plan to report their results and make refinements to their processes, and then proceed to phase two, which will be a year-long trial with six subjects.
Having Palipana as a test subject gives the team unique insight.
“Dinesh gives us an opinion and brings in lots of expertise from a medical perspective and also from the perspective of an individual with spinal cord injury so we also understand what are some of the additional constraints we need to undertake,” Pizzolato said.

That enables his feedback to be more precise, said Dr Ana de Sousa, an expert in using robotics for rehabilitation.
“It’s funny to see our conversations, like we’re trying to find out when he’s the patient, when he’s the boss of the thing,” she told create.
“He doesn’t know the engineering aspect of it, but he knows the overall purpose, and overall goal … his feedback is a little more on point. He knows more where he wants to get.”
Taking steps
The BioSpine project uses existing technologies but combines them in unprecedented ways in hopes of making a breakthrough that is not yet possible. That, Pizzolato said, is what distinguishes it from similar work being conducted overseas.
“Our foundation is solid,” he said. “What we’re doing is putting everything together, plus adding a computational model of the person to really coordinate the rehabilitation devices.” The BioSpine team comprises engineers, doctors, physiologists, pharmacologists and more in pursuit of a genuinely multidisciplinary goal.
“The thing with medicine is that it’s so slow to adapt to change,” Palipana said. “Engineers are so solution-focused and they’re practical as well, which I have found to be really good because we are able to identify all these different problems and the guys in our team drive solutions.”
And though the team is yet to report results, everyone create spoke to was optimistic about the technology’s future prospects. If the round two trials go well, Pizzolato expects the therapy to be used outside a university setting by the end of 2023.
“We don’t want it to remain a nice exercise that we do at the university and never goes out to the public,” he said. “Eventually, if the technology goes in clinics, you need to get the clinicians on board.”
Diamond concurs.
“We can’t service large numbers of people in the community within the university long-term. It’s not sustainable,” she said. “The idea is that you want accessibility; you want effective therapy to be accessible to all.”
When asked about his next steps, Palipana’s response is direct — and literal.
“To take steps,” he said.
“That would be the dream actually. It’s an audacious dream, but that’s what we’re working towards. To give people that opportunity.”


This story is inspiring. I am a retired civil engineer diagnosed with MS in 2012, with the controlling lesion at C4 in my spinal cord. I battle to continue walking, the alternative being a wheel chair.
I don’t know whether I can be of use, perhaps as a patient.
Please feel free to contact me if you would like to.
Kind regards,
Peter Glen
An inspirational story! I’m having SCI and currently on wheelchair for mobility. I would like to take part in the research, please contact me if there is any way that I can be of use.
Regards
Deepak
The fact that this program aims to transform an individuals life after misfortune can not be over stated – this sort of progressive work puts to shame some of the public grants given to unviable and idiotic programs – a really close friend is paralysed from the chest down after a motor vehicle accident and in a similar situation as Dinesh – he’s resolve and determination is second to none and I can see that the out come of this program will benefit not only him but everybody around him. Keep the good work going – our support is offered in any way we can help.
This is a fantastic research program. This is a showcase of what engineering is about, helping people and making their lives better.